
#NACFC2016 – Colonoscopy Recommendations for Colon Cancer Screening in CF Patients



In a recent talk titled “Implementation of Colorectal Guidelines,” Alexander Khoruts, MD, from the University of Minnesota, discussed recommendations for an effective screening for colorectal cancer in patients with cystic fibrosis (CF).
The talk was presented at the 30th Annual North American Cystic Fibrosis Conference Oct. 27-29 in Orlando, Florida.
Patients with cystic fibrosis are seeing positive changes, such as longer lifespans, but new complications have also emerged, such as an increased incidence of colon cancer.
Measures to ensure early detection of colorectal cancers and the removal of adenomatous polyps (gland-like growths that develop on the mucous membrane that lines the large intestine and carry a higher chance to become cancerous) have been efficiently employed in the general population.
While this suggests the same strategy may prove beneficial in CF patients, Khoruts emphasized important considerations so that an effective colorectal screening program is established. These include:
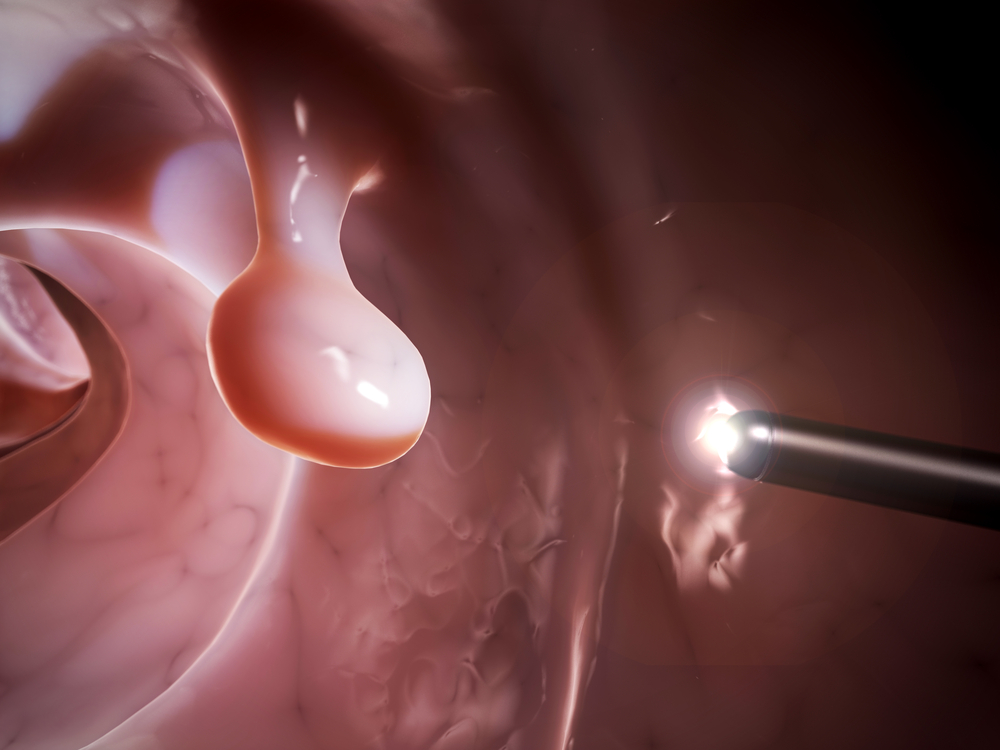
1) A high quality preparation of colonoscopy sample is essential so a doctor can identify and remove a polyp. A colonoscopy test is used to look inside our bodies for small, wart-like growths – the polyps – that can turn to cancer. But obtaining a sample is harder in CF patients than in others due to more adherent fecal material and underlying constipation. Khoruts suggested that split preps from a colonoscopy are better than single, large-volume preps.
2) Khoruts highlighted that gastroenterologists, even in large CF centers, are not fully aware of the link between cystic fibrosis and significantly higher chances of colorectal cancer. Also limited is their knowledge of the special challenges associated with a colonoscopy in CF patients. Therefore, it is important that gastroenterologists become familiar with these difficulties so that enough time is reserved for CF patient examinations. CF patients usually undergo more difficult colonoscopies, and time is necessary to allow doctors to examine multiple polyps (which are likely to arise in CF).
3) Preparation for examination of CF patients is intimately linked to a patient’s medical condition. It’s reported that patients feel less pain and discomfort after a colonoscopy when the bowel is insufflated with carbon dioxide instead of room air. But a patient with poor lung function undergoing a lung transplant evaluation should probably be first screened by a fecal immunochemical test (FIT) for colorectal cancer, which tests for hidden blood in the stool, which can be an early sign of cancer.
Khoruts also emphasized that the respiratory status of the patient should be considered in planning sedation for colorectal examinations, whether it is performed by the gastroenterologist or assisted by the anesthesiologist.



